



Many ocular conditions may cause watery eyes, for example, in response to emotions or cold, windy weather, but as soon as the causing factors disappear, the watering stops. Persistent watery eyes on the other end can have many causes, including allergies and infections.

Watery Eyes Symptoms
Constant tearing is what brings the patient to the doctor’s office and involves most often female patients in their 50s. A common complaint is that “tears run down the cheek,” or “I have to dub my eye more than 10 times each day”.
Often, the lacrimal sac enlarges, and the patients palpate a soft induration between the eye and the nose; other times, they have chronic secretions and mattering, indicating chronic inflammation.
Occasionally, a blocked tear duct can cause acute inflammation of the sac known as acute dacryocystitis that requires immediate attention.

What Causes Watery Eyes?
The most common condition of watery eyes is a blocked tear duct, which is the channel through which tears are drained into the nose. There are no medicines or medical treatments that can cure it.
A medical consult with a specialist in lacrimal surgery (usually an ophthalmologist with sub-specialty training in oculoplastic surgery) is required to establish the appropriate diagnosis and rule out other conditions.
Watery Eyes Diagnosis
Irrigation of the tear duct with a syringe is necessary to confirm the diagnosis in most cases and can be performed at the time of the first consultation.
Once the diagnosis of PANDO (Primary Acquired Naso-lacrimal Duct Obstruction) is established, the final treatment is a surgical procedure called dacryocystorhinostomy and can be performed through a small skin incision over the lateral part of the nose that leaves an invisible scar, is performed under local anesthesia with monitored intravenous sedation and in an outpatient center (External Dacryocystorhinostomy).
Dacryocystorhinostomy (DCR) can also be performed through a nasal approach with the endoscope, thus avoiding the external scar (Endoscopic DCR).
The success rate of this procedure is superior to 95% in most cases; the 5% of residual tearing can be further treated through an endoscopic revision of the surgical site, approaching the 100% success rate.
Surgical Technique




DIFFICULT OBSTRUCTION? FAILED THE PREVIOUS SURGERY?
There are anatomical variations of the site of the obstruction that makes surgery more complex and less predictable.
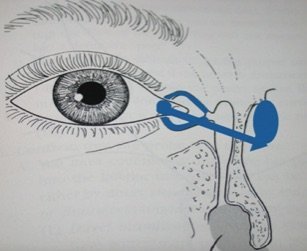
One example is when the obstruction occurs before the lacrimal sac, so-called pre-saccal obstruction, caused by internal scarring of the lacrymal canaliculi present in the eyelids. A standard DCR cannot be performed in these conditions, and a more ‘complicated’ procedure is indicated. A permanent tube is placed between the eye and the nose, by-passing the pre-saccal obstruction.
The stent is positioned through a nasal endoscopic approach and has no external scar. This procedure is also indicated for patients with multiple DCR failures.
Diagram showing the obstruction in the eyelid canaliculi and the direction of the by-pass (arrow) from the eye to the nose.
The tube is not visible externally, and it is well tolerated by the patients.
Example of a patient with Jones’s tubes in both eyes; the tube isn’t visible unless the eyelids are everted:
